What is Medical Data De-Identification?
Medical data de-identification involves removing or masking personal details of patients from their health records, such as names, dates, location details, ID numbers, and faces in photos or biometrics. This breaks the link between the medical data and the individual, protecting privacy while allowing AI developers and researchers to use the information for model development. Rather than relying on a one-size-fits-all approach, de-identification encompasses a range of techniques that are applied based on the type of sensitive information involved, organizational privacy policies, regulatory requirements, and the intended use of the data.
Why De-Identification is Required
- Protection of Patient Privacy and Confidentiality: Medical data often contains personally identifiable information (PII) and protected health information (PHI). De-identification removes or obscures these elements to prevent unauthorized disclosure of patient identities.
- Legal and Regulatory Compliance: Health information containing personal identifiers that are linked to the individual who is the subject of the information is protected under federal and state laws such as HIPAA, FDA regulations, GDPR, and others. De-identification helps organizations comply with privacy regulations by reducing the risk of exposing personally identifiable information during data processing, sharing, and AI development.
- For Robust AI and ML Model Development: Access to large, comprehensive, and diverse real-world datasets is essential for improving patient outcomes, enhancing diagnostic accuracy, advancing research, and developing reliable AI and ML models. De-identification allows researchers and AI developers to use medical data while reducing risks to patient privacy.
- To Facilitate Secure Data Sharing: Collaboration among hospitals, research institutions, and AI developers often requires access to clinical data. De-identification makes the sharing of such datasets legally and ethically permissible.
- To Maintain Analytical Utility: Simply stripping identifiers without preserving data relationships can significantly reduce the value of clinical datasets. Effective de-identification maintains the analytical value of clinical datasets by preserving temporal relationships, patient cohorts, and cross-document relationships.
- To Meet Audit and Governance Requirements: AI models trained on healthcare data are subject to regulatory security and governance requirements. De-identification ensures that training, validation, and testing datasets adhere to privacy requirements, while documented methodologies, validation metrics, and audit trails provide evidence of responsible data use during audits and compliance reviews.
Aligning De-Identification Strategies with Regulatory Requirements
De-identification is at the intersection of technical, legal, and regulatory considerations. The process is shaped by privacy regulations, legal requirements, acceptable risk levels, and regional compliance obligations. For example, European law (GDPR) has much stricter rules for anonymization than US healthcare law (HIPAA). Therefore, it is important to know your legal and compliance rules that apply to your data, geography, and intended use before you start building your data pipeline or removing information.
Clinical Data De-Identification Challenges
- Identifying PHI Across Diverse Data Types
Clinical data is available in multiple formats, including medical images, formatted tables, free-text clinical notes, audio recordings, and DICOM metadata. Sensitive information can exist in any of them, making complete identification challenging. - The Privacy-Utility Tradeoff
De-identification often requires masking, removing, or replacing sensitive information, which can reduce the usefulness of the data for downstream analysis. It is challenging to protect patient privacy while preserving the clinical value of the dataset. Excessive suppression and complete masking directly compromise the data usefulness for analytics and AI model training, while insufficient de-identification increases re-identification risks. - Preventing Re-Identification Risks
Even after the removal of direct identifiers, combinations of partial identifiers such as age, location, rare conditions, and treatment records can potentially be used to re-identify individuals. The growing sophistication of AI and data-linkage techniques further increases the risk of re-identification. - Detecting PHI in Medical Images
Medical images may contain identifiers as burned-in text embedded directly in pixel data. Automatically detecting and removing such information from metadata requires specialized OCR, computer vision, and image-processing capabilities. - Managing Multilingual and Mixed-Language Data
Most de-identification tools are designed primarily for English-language corpora. However, healthcare records often contain multiple languages (e.g., Hindi-English mixing in Indian hospitals, French in Canadian records), abbreviations, and code-mixed text, making PHI detection significantly more challenging. - Regulatory Variability Across Jurisdictions
Clinical data is governed by overlapping and sometimes conflicting regulations — such as HIPAA, GDPR, FDA requirements, and regional healthcare privacy laws. Datasets anonymized under one framework may still be classified as identifiable under another, complicating cross-border data sharing and global research collaboration. - Ensuring Accuracy at Scale
Even a small number of missed identifiers can lead to compliance and privacy risks. Achieving consistently high accuracy across millions of records requires robust quality assurance processes, validation metrics, and comprehensive audit trails.
Types of De-Identification Techniques
There is no single de-identification technique that aligns with every dataset or regulatory context. The right de-identification technique depends on the applicable legal framework, data modality, and re-identification risk. The ideal approach involves combining multiple methods—such as redaction for highly sensitive identifiers, tokenization for names and IDs, and date generalization or shifting for temporal data—to balance privacy, compliance, and data utility.
1. Safe Harbor De-identification
It’s a HIPAA-defined rule-based technique that requires the removal of 18 categories of identifiers, including names, phone numbers, social security numbers, medical record numbers, and dates linked to a patient. Data from which all 18 identifier categories have been deleted is considered de-identified under HIPAA’s Safe Harbor provision.
Best for: Regulatory compliance and data sharing.
2. Expert Determination
Experts assess the dataset and certify that the risk of re-identification is minimal. Unlike Safe Harbor, this approach allows certain data elements, such as dates, geographic information, etc., to be retained if the re-identification risk is sufficiently mitigated.
Best for: Research and AI model development where data utility must be preserved.
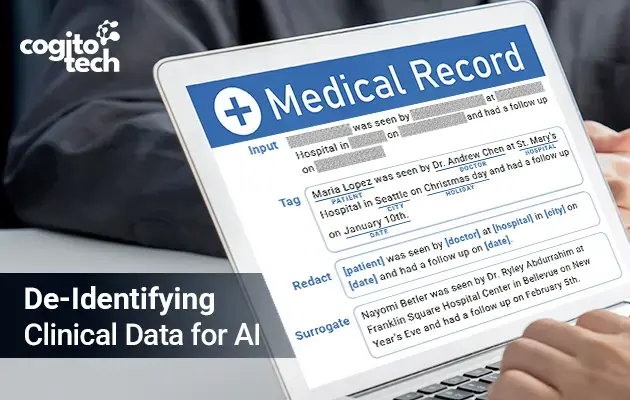
3. Redaction (Suppression)
Redaction removes sensitive fields or visual elements from the dataset.
Example:
Patient Name → Removed
Phone Number → Removed
For: Strong privacy protection.
Limitation: Information loss.
4. Masking
Medical data masking is the process of partially obscuring sensitive values while preserving some context. It replaces real details with fake or scrambled values.
Example:
– Phone: 75765XXXXX
– Email: s***@gmail.com
Advantage: Retains usability.
Limitation: Room for re-identification risks.
5. Anonymization
All direct identifiers and indirect inferences must be addressed so that re-identification is appropriately controlled. When data is irreversibly anonymized and individuals can no longer be identified, it generally falls outside the scope of GDPR requirements.
Example:
– Name removed
– Identifier key destroyed
– Quasi-identifiers generalized
Advantage: Highest privacy protection.
Limitation: Often reduces data utility.
6. Pseudonymization
Pseudonymization replaces direct identifiers with artificial identifiers or codes while keeping a controlled re-identification key.
Example:
– Patient ID: John Smith → PT-84729
A separate key is stored securely and can re-identify the patient if authorized.
Advantage: Enables longitudinal tracking.
Limitation: Re-identification risk continues.
7. Tokenization
Replaces sensitive values with random tokens that have no mathematical relationship to the source value. Tokenization is often used to support pseudonymization and enable controlled data linkage across systems.
Example:
– MRN 123456 → TK-9A7F2
The mapping is stored separately in a secure token vault.
Advantage: Strong protection while maintaining database relationships.
How Cogito Tech Leads Medical Data De-Identification
Cogito Tech’s Medical AI Innovation Hub brings together board-certified clinicians, healthcare specialists, and compliance experts to support accurate, privacy-compliant clinical data de-identification through expert validation, audit-ready workflows, and secure data handling practices.
De-Identification Services
PHI/PII Detection and Validation: Identify, mask, and remove sensitive identifiers from clinical records, documents, and healthcare datasets using AI-assisted workflows and expert review.
Clinical Text De-Identification: Detect and redact patient identifiers from physician notes, discharge summaries, pathology reports, and other unstructured medical text.
Medical Imaging De-Identification: Support the removal of PHI from DICOM metadata, burned-in text, and other identifiable imaging elements.
Auditability and Traceability: Maintain comprehensive review records, audit trails, and workflow documentation to support regulatory and quality requirements, including 21 CFR Part 11-aligned processes.
Custom AI Enablement Services
Training Data Preparation: Prepare de-identified datasets for clinical NLP, computer vision, multimodal AI, and healthcare analytics.
PHI Annotation and Model Evaluation: Annotate PHI entities and assess model performance to strengthen detection accuracy and reliability.
Human-in-the-Loop Model Refinement: Provide continuous expert feedback and validation to improve model outputs and adapt to evolving data requirements.
Scalable Clinical Expertise: Deploy domain-trained annotators, healthcare specialists, and quality reviewers to support large-scale de-identification initiatives across diverse clinical data types, languages, and healthcare domains.
Conclusion
As clinical datasets grow more complex and regulatory scrutiny intensifies, missed identifiers, inconsistent methodology, or incomplete audit trails can compromise both patient privacy and model integrity. Cogito Tech’s Medical AI Innovation Hub solves this directly — combining board-certified clinical expertise with partner annotation tooling and audit-ready workflows across every stage of the de-identification pipeline, from PHI detection in unstructured clinical text to DICOM metadata sanitization and specialist-in-the-loop model refinement — so medical AI teams can scale faster without compromising privacy or compliance.